Spasticity management in children.
Why does it matter so much?(IT’S ALL IN THE HIPS)
When children are born, their joints and bones are not fully developed. These joints take shape as the child grows, starts to use them, and put weight on them. The hip is a ball and socket joint. Before children start standing and walking, the socket is still flat, it forms slowly and takes shape over time with standing and walking.
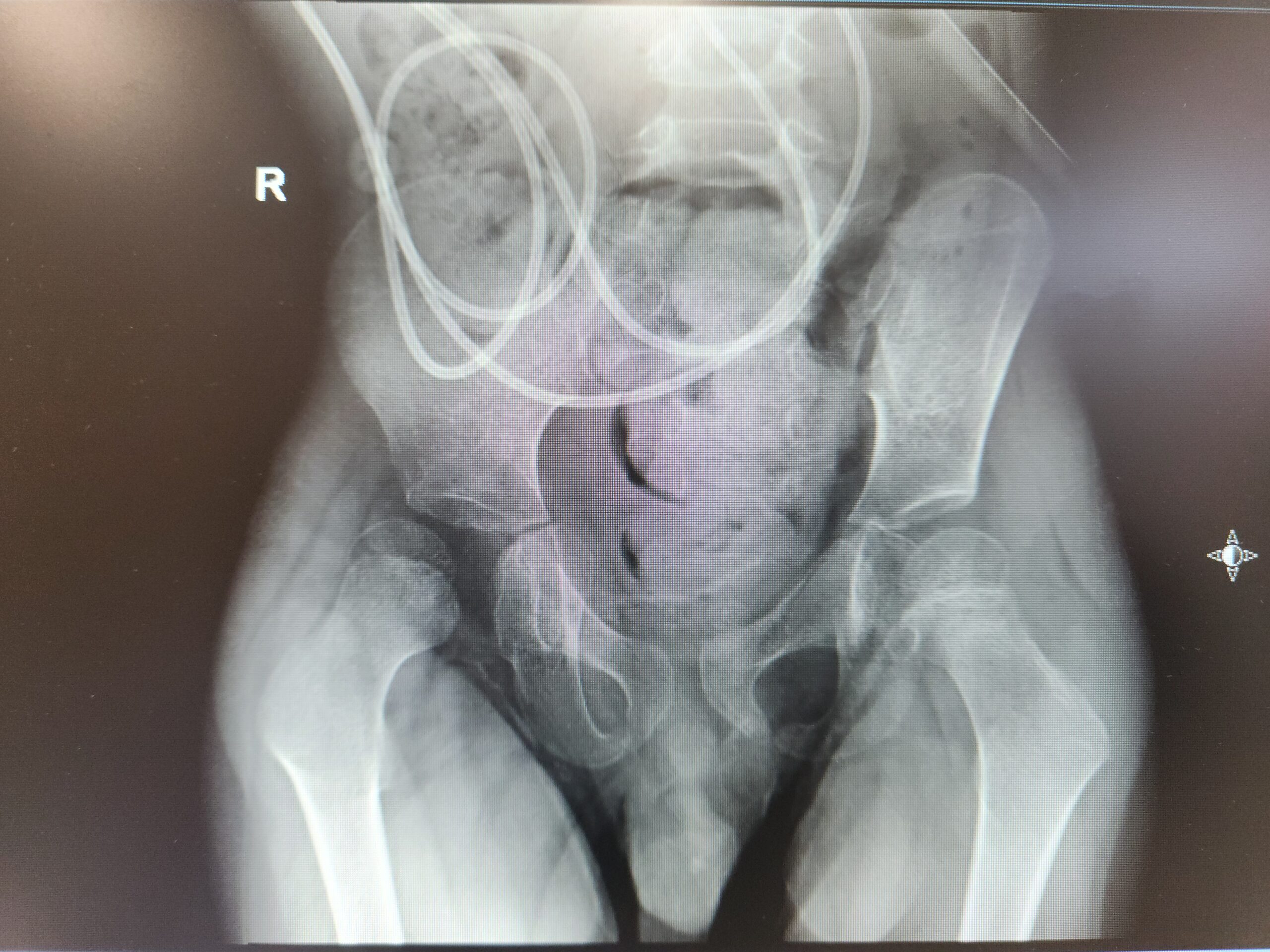
As you can imagine, hip development would be difficult if the child never starts standing on their own due to any condition affecting their gross motor development, such as children with spina bifida, cerebral palsy, or spinal muscular atrophy. With the hip socket shallow or flat, the hip bone itself is free to move and migrate, usually outwards and backward. So …..any child who is not able to walk “on time” is at risk for hip subluxation or migration. Children with cerebral palsy causing spasticity/tightness around the hip muscles are at even higher risk as the tight muscles tend to pull on the bones, accelerating the hip deformity.
For this reason, aggressive treatment targeting the hip muscles, flexors, adductors and medial hamstrings, should be prioritized. This is typically a multi-disciplinary affair. Stretching with PT, splinting (hip adductor wedge, knee extension splints), serial casting for the calfuscles, oral or local medications to relax the muscles, and, most importantly, initiating a standing program using standing frames or gait trainers (depending on the child’s ability) are all essential components to an effective treatment program.
All of this is done to prevent hip migration and dislocation as much as possible. Hip dislocation can cause pain, difficulty with positioning, pressure ulcers, and contribute to spine asymmetry (neuromuscular scoliosis). Every treatment should have a clear goal and plan in order to achieve it.